Newsletters: 2000
Contents:
- Change is in the Air: An Editorial
- Bill H-594 -200 - Vermont General Assembly
- From the Commissioner of Health: State of Vermont
- It's a Crazy World! Editorial
- Letter to Senator Jeffords
- Letter From Senator Jeffords
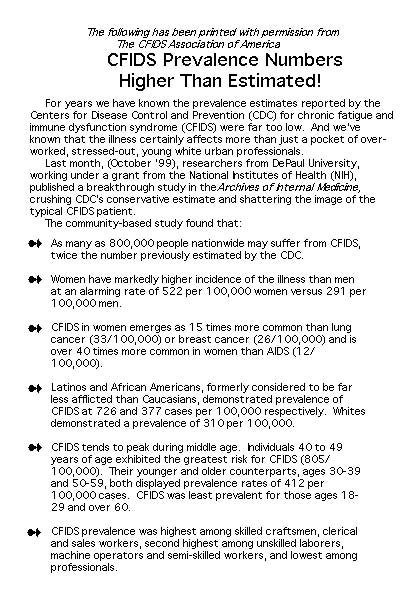
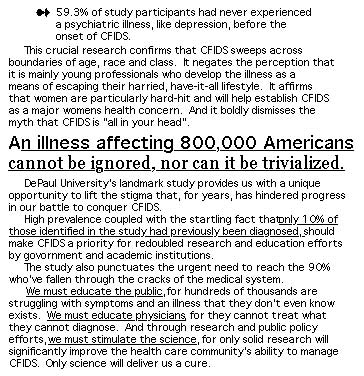
- CFIDS Prevelence Higher than Expected
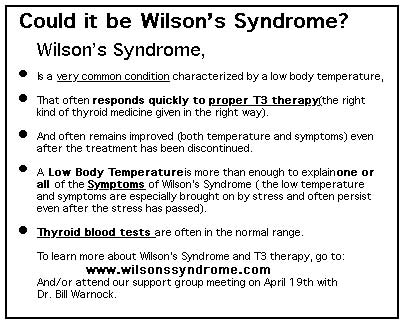
- Could It be Wilson's Syndrome?
- Overlapping Disorders by Rochelle Reome
- The Virus Within: A Book Review
- Reflections by Rachel Sherman
- The Future of Our Support Group
- "I Remember Me" by Kim Snyder
Change Is In the Air! An Editorial
Many of us are familiar with the endless trek from doctor to doctor to doctor trying to find an answer, a cure, an alternative treatment, something/anything, to this god-awful disease that has kept us home-bound and sick and doesn't go away. I have been at the receiving end of the Association's 800 number for almost four years and I've heard the stories over and over again as though they were one. I've talked to hundreds of people. I've heard the search for words and the struggle for descriptions as we try to explain the fatigue, the brain fog, or the overwhelming exhaustion that happens when we try to accomplish common household chores, (God-forbid we try to raise children). I hear about the headaches and repeated sore throats, the terrible joint pain, the restless anxiety and the non-restorative sleep. And then I hear about the doctor's visits. How after months of investment in a physician and months of tests that turn up negative, chronically ill people are sent-packing with nowhere to turn, nowhere to go and more questions than ever before. "It's all in your head." "You just need some exercise." "There's nothing I can do." "Go home and rest." (As if there were a choice.) "You're lazy."
I hear the stories as if they were one.
Occasionally I hear a spark of hope. But then, even when I do learn of a physician with insight, compassion and a willingness to explore treatment options, he or she is invariably outside the realm of traditional insurance, and might as well be on the moon to patients who have lost their job and exhausted their savings after years of being ill. Within the confines of managed care in Vermont I don't think there's a single physician, not even one, who has even an elementary grasp on the recovery process with CFIDS. If you can show me to be wrong, please call or write. Please.
Then there are the physicians who claim to have an understanding of this disease, who readily share this knowledge with their cohorts, but then have closed their practices to any new CFIDS patients. Then when asked for referrals, they send desperately ill people out of state, where after the most horrendous of runarounds they're discharged with the same litany of excuses. Every time this happens, and I mean EVERY time this happens, the symptoms are exacerbated and the disease is substantially prolonged. These actions make people worse.
One of our more pressing needs is to educate physicians in Vermont. We need to teach as many as will listen that this disease is real, it's debilitating and it's prolonged. We need to show that while there currently is no known cure, there are many effective treatments and people's health can be improved. Proper diagnosis is just the beginning. Recovery requires recognition, attention to dietary and nutritional protocols, blood work that focuses on specifics, and substantial lifestyle adjustments. This takes direction and requires a partnership between the doctor and the patient. We need partners.
Our goal is to have a list of physicians who understand this disease, who have a grasp of the recovery process and who are readily available through conventional insurances. Why should this be so difficult?
We began this process in January by introducing legislation that directs the Vermont Department of Health, in conjunction with the VT CFIDS Association, to educate the medical community about CFIDS. A copy of our bill is on page four. We are indebted to Rep. Patricia Doyle of Richmond who introduced this bill and is our guiding force. We also owe special thanks to Reps. Jim McNamara of Burlington and Anne Pugh of So. Burlington.
Since then, we have received a copy of an internal letter from the Commissioner of Health that agrees to our request! (See page 5.) As a result, the legislation has been put on hold, and we have initiated a dialogue with the Department to fulfill our requests. Anyone who wants to be a part of this process is welcome, your input is imperative. We can make a difference.
Change is in the air.
The longest journey begins with a single step.
Rik Carlson
From the Commissioner of Health...
The following is excerpted from a memorandum to Rep. Paul Poirier, Chairman of the House Health and Welfare Committee, from Jan K. Carney, MD, MPH, Commissioner of the Vermont Department of Health regarding Bill H.594 - Chronic Fatigue Syndrome.
This is being printed with permission from Rep. Poirier.
January 25, 2000
"In follow up to my testimony last week regarding(this) bill, the department of Health can provide public and professional information on (this) issue. While not carrying out every detail of the proposed legislation, we will attempt to address the intent and spirit of (this) proposal. In the area of chronic fatigue syndrome, we will work in collaboration with the Vermont CFIDS Association, Inc., along with health care providers with expertise in chronic fatigue syndrome to provide information to the public and also to health care professionals in Vermont. This would include information from the Centers for Disease Control and Prevention, specifically their web site, to provide health professionals with current research and guidelines for chronic fatigue syndrome.
Such information could go out through our existing publications or the creation of a fact sheet that includes the web site for CDC, and phone numbers for individuals who wish to participate in available support groups. In addition, the Department will work closely with such professional organizations as the Vermont Medical Society and the Vermont State Nurses Society such that this information could be integrated as part of any continuing medical education efforts.
We would see these educational efforts occuring within our current budget and responsibility located in our division of Health Improvement. The committee's idea of a resolution in (this) area is an excellent one and would help to further focus public attention in (this) area.
It's a Crazy World!
In the political world of disease, for some unearthly reason, CFIDS has been treated as a joke by the Centers for Disease Control (CDC) and the National Institutes of Health (NIH). Derogatory fabrications about this disease were actually taped to the office walls of some of the top level researchers at the CDC. Valid research was ignored, project grants were repeatedly denied, and to be involved in CFIDS-oriented study has been the kiss-of-death for career-minded physicians and researchers. For years on end, money authorized by Congress (because of the outcry of their constituents) for research into CFIDS was diverted to other projects at the whim of high powered bureaucrats. Recently the CDC admitted diverting millions of dollars away from CFIDS studies as a pattern of behavior. They apologized. The following letter was sent to Vermont's Congressional delegation last October. This in turn is followed by Senator Jefford's response.
Dear Senator Jeffords,
As you may be aware, last
spring the Department of Health and Human Services' Inspector General
found that the Centers for Disease Control and Prevention (CDC) had misdirected
funds for chronic fatigue syndrome (CFS) research and lied to Congress
and the American people about it. Although CDC has apologized for its
mismanagement of CFS funds and has stated that the funds will be restored
to the CFS research program, significant problems remain at the CDC and
other DHHS agencies.
The people responsible for the diversion of funds from CFS into other
programs remain in position at CDC and maintain control over the CFS program's
operation.
DHHS Secretary Donna Shalala has been virtually silent on the IG's findings, as have other DHHS officials. Any response they have made is merely a restatement of CDC's letter of apology.
There have been no assurances that DHHS is taking CFS seriously as a disabling illness or important health concern, despite new data from CDC which shows that more women have CFS than have lung cancer, HIV, or AIDS.
The National Institutes of
Health (NIH) has not changed its long standing indifference to CFS research.
Despite the generous increases Congress has given NIH in recent years,
CFS research funding actually decreased 11% from FY97 to FY98. The total
NIH investment in CFS research in FY98 was $6.4 million, just $12.80 for
each of the 500,000 American men, women, and children who have CFS.
The CFIDS Association of America, the nations leading organization working
to conquer chronic fatigue and immune dysfunction syndrome (CFIDS), has
tried to work with the federal health agencies to correct these problems,
but has met with resistance and apathy from many of those who are charged
with protecting the nation's health. The problems with the federal government's
CFS research program are grave and deserving of increased scrutiny. A
hearing in the Health, Education, Labor and Pensions Committee on the
federal government's management of CFS research would shed light on the
problems and send a message to the federal health agencies that Congress
is serious about its annual requests for increased attention and research
on CFS.
As one of at least 500,000 Americans with CFS who are depending on federal resources to help scientists to discover the cause, treatment, and cure for CFS, I ask that you take my request seriously and schedule a hearing this fall to examine the government's attention to CFS research and policy.
Thank you for your consideration of this important matter. If you have any questions about the diversion of funds or any other CFS related matter, please contact Mary Beth Buchholz of The Sheridan Group at 202-462-7288.
Sincerely,
Rik Carlson
Senator Jefford's response follows:
United States Senate
COMMITTEE ON HEALTH, EDUCATION,
LABOR AND PENSIONS
December 16, 1999
Dear Rik,
Thank you for contacting me to express your views about chronic fatigue syndrome (CFS) and the failure of the Centers for Disease Control and Prevention (CDC) to focus the appropriate research resources to learn more about this debilitating disease. I share your concern about this critically important issue and I would like to take a moment to provide you with some recent developments and to share my views.
As you may know, a May 1999 report by the Inspector General of the Department of Health and Human Services (HHS) found highly questionable charges regarding funding for the Chronic Fatigue Syndrome (CFS) program during fiscal years 1995 through 1998. The Inspector General report attributed these questionable charges to deficiencies in the CDC internal control system regarding the handling of direct and indirect costs. In addition, CDC officials provided inaccurate information to the Congress regarding the use of CFS funds, and have not supported the CFS program to the extent recommended and encouraged by the Congress.
I was gravely concerned to learn of these activities and have directed CDC to provide my office with a full account of how they will restore the estimated $12,900,000 to CFS research, and details on how it will pursue an aggressive research plan. The agency has also been directed to develop public education programs, educate primary care providers on the detection, diagnosis and treatment of CFS, develop surveillance projects on children and adolescents with CFS and conduct an interdisciplinary reassessment of the case definition for CFS. In addition, CDC will need to determine the pathogenesis of CFS, estimate its incidence and prevalence, describe its natural history, identify risk factors and diagnostic markers and develop control strategies. Finally, the agency has been directed to participate in the HHS' Coordinating Committee on CFS.
The HHS CFS Coordinating Committee met in mid-November, together with patient representatives, and established the objectives of the CDC's CFS program. The agency has made the commitment to: 1) estimate the magnitude of the problem in the U.S. (e.g., prevalence and incidence); 2) evaluate the possibility that CFS is a symptom complex that could represent a final common response to a variety of insults; 3) define the natural history of CFS; 4) identify risk factors and diagnostic markers; 5) provide current, appropriate technical information on CFS to government agencies, public health officials, health care providers, patients, and the public, and ultimately; 6) develop control and prevention strategies.
In addition to the above activities, you should know that a complete review of the CDC's actions has been undertaken by the General Accounting Office (GAO) which is expected to release its report in the spring of 2000 and a request has been made to Attorney General Janet Reno to make a determination as to whether agency's misallocation of CFS funds warrants a criminal investigation.
I want to assure you that I am pursuing this issue aggressively. I intend to watch closely the outcome of the GAO report and the Department of Justice investigation and will continue to require CDC to keep me informed on the progress it is making on CFS.
Thank you again for contacting me. I will continue to follow this issue closely and do what I can to ensure that the federal agencies responsible for CFS research fulfill the mission assigned to it by the Congress. Please keep in touch on this or any other matter of importance to you.
Sincerely,
James M. Jeffords
Overlapping Disorders
by Rochelle Reome

The Future of Our Support Group
Finis